|
BACKGROUND
Clubfoot is the most common congenital orthopaedic anomaly occurring in 1 in 1,000 live births. The affected foot is in an excessive down-and-in position (equinovarus) with a high medial arch (cavus). Without treatment, clubfoot can result in long-term disability and pain. Standard of care for treatment of clubfoot is the Ponseti method, which consists of serial manipulation and casting, and a percutaneous Achilles tenotomy to correct the foot shape. The correction is then maintained using a Foot Abduction Brace (FAB). The wear schedule for the FAB is 23 hours per day for three months, then at night (12 hours/day) until five years of age. Ideal position for the clubfoot in the brace is approximately 10 degrees of dorsiflexion, and 60 degrees of external rotation with the feet held shoulder-width apart.
FABs consist of two ankle-foot orthoses (boots) connected to a bar. To maintain the ideal corrective foot position, FABs must hold the feet in a dorsiflexed, everted, and externally rotated position at shoulder-width distance apart. The standard bars are straight and restrict independent knee and hip movement. Some studies report that parents find the FABs with a straight bar uncomfortable for their children, and approximately 35% of clubfoot patients do not comply with the prescribed bracing schedule. Bracing is critical for good outcomes, as lack of brace tolerance and inadequate time in brace are shown to increase recurrence rates by 5-to-17 times.
DESCRIPTION OF INVENTION
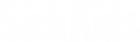
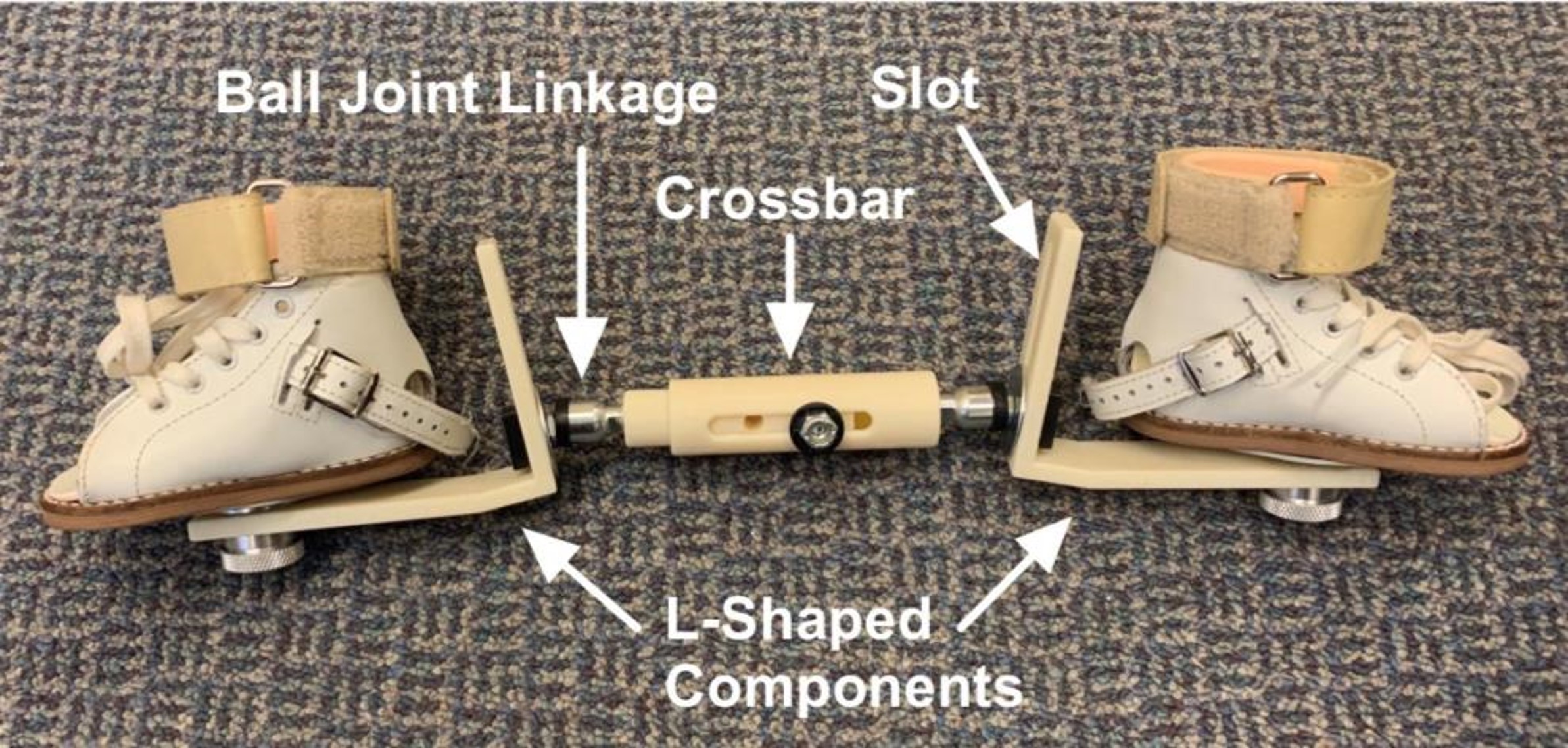
Our novel device is a new style of dynamic bar to be used for foot abduction bracing in clubfoot treatment. Our design consists of a straight crossbar attached to two sliding L-shaped components that fix the foot at each end of the bar. Each L-component is attached to the crossbar via a ball-joints linkage, which combined with the vertical slot in each L-component, allows independent extension and flexion the knees and hips and 30 degrees of internal/external rotation of the hips. This bar has the potential to greatly improve child comfort and parent experience with clubfoot bracing by increasing patient's leg motion, while maintaining the ideal corrective foot position. With better brace tolerance, risk of recurrence can be minimized and clinical outcomes, as well as patient and parent reported outcomes, improved. The added mobility provided with our dynamic bar may enable patients to maintain or gain leg muscle strength during use, possibly further decreasing risk of clubfoot recurrence due to muscle imbalance and weakness of the peroneal everter muscles.
COMMERCIAL ADVANTAGES
- Validation: Competitor products lack the rigorous clinical studies we have begun for the Dynamic Foot Abduction Bar.
- Increased mobility resulting in increased compliance.
MARKET OPPORTUNITY
Up to 200,000 infants are born with clubfoot every year, and so we can expect that approximately 800,000 patients are using an FAB at any given time if worn until age four. Given that 35% of patients do not comply with the prescribed bracing schedule, as many as 280,000 children are struggling with current models and may benefit from use of our novel dynamic bar.
There are few dynamic bars for FABs currently on the market. A popular design, the Dobbs Bar, contains spring-loaded hinges that allow independent leg movement in the coronal plane, and return the patient's feet to the ideal corrective position when the legs relax. Studies suggest that this independent mobility is directly correlated with greater comfort, increased compliance and lower recurrence. However, since patients can over-power the springs, the Dobbs bar enables intermittent loss of the ideal foot position by allowing plantarflexion and inversion of the feet. This might also strengthen the clubfoot deforming muscles, the tibialis posterior and the plantarflexors of the feet, possibly worsening muscle imbalance and increasing risk of recurrence.
Our novel dynamic bar design has clinical and commercial advantages over existing hinged bars, as it allows for independent leg movement, while only allowing foot and ankle movement in the directions of increased dorsiflexion, external rotation and eversion. It therefore prevents all foot positions which may worsen the deformity, contribute to foot muscle imbalance, or increase risk of recurrence. There are no Canadian-made FABs on the market, and current projections suggest that this novel dynamic bar will be less expensive to produce than the Dobbs Bar. Our bar may therefore present a homegrown option that is attractive to both patients and Canada's provincial health care programs. If cost remains low, this bar would also be competitive in a global market, particularly for low-and-middle-income countries where 80% of clubfoot cases exist.
Each child will receive their first bar at three months of age and require a larger bar at ages 12–18 months and 3–4 years.
DEVELOPMENT STAGE
Five prototypes developed using 3D printing for use in an upcoming clinical trial. The clinical trial is expected to be completed by December 2022 and we hope to have statistically significant data by Q1 2023.
PATENT STATUS
A US Provisional patent has been filed for the Dynamic Foot Abduction Bar.
|
|